In response, the Flint Area Study (FASt)
- A longitudinal multi- and inter-generational study of risk and resilience.
- Designed to serve as a comprehensive data resource that will inform local policy and interventions.
- Will measure the epigenetic and behavioral impact of physical- and social-environmental exposures.
Phase 1 Goal: Generate the sampling frame for 400 Flint households (350 citywide + 50 oversample in North Flint), for a total of approximately 1,000 residents.
METHODS:
Scouting was completed with eight raters. Raters were Flint area residents, selected because of their comfort and familiarity with the city, that were trained as data collectors. Pairs of raters assessed block faces based on defined signs of habitation (e.g. illumination, shoveled snow) and their subjective reasoning. Raters were instructed to not discuss inhabitation while conducting assessments. Households were considered inhabited when at least one rater indicated such.
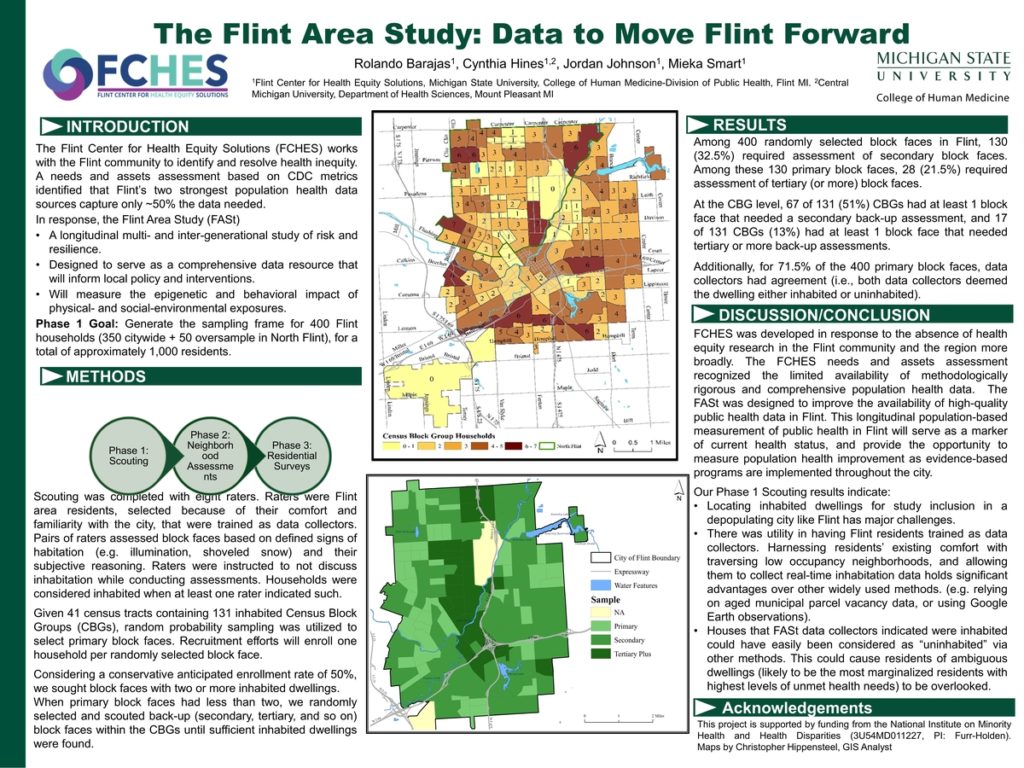
Given 41 census tracts containing 131 inhabited Census Block Groups (CBGs), random probability sampling was utilized to select primary block faces. Recruitment efforts will enroll one household per randomly selected block face.
Considering a conservative anticipated enrollment rate of 50%, we sought block faces with two or more inhabited dwellings.
When primary block faces had less than two, we randomly selected and scouted back-up (secondary, tertiary, and so on) block faces within the CBGs until sufficient inhabited dwellings were found.
RESULTS
Among 400 randomly selected block faces in Flint, 130 (32.5%) required assessment of secondary block faces. Among these 130 primary block faces, 28 (21.5%) required assessment of tertiary (or more) block faces.
At the CBG level, 67 of 131 (51%) CBGs had at least 1 block face that needed a secondary back-up assessment, and 17 of 131 CBGs (13%) had at least 1 block face that needed tertiary or more back-up assessments.
Additionally, for 71.5% of the 400 primary block faces, data collectors had agreement (i.e., both data collectors deemed the dwelling either inhabited or uninhabited).
DISCUSSION/CONCLUSION
FCHES was developed in response to the absence of health equity research in the Flint community and the region more broadly. The FCHES needs and assets assessment recognized the limited availability of methodologically rigorous and comprehensive population health data. The FASt was designed to improve the availability of high-quality public health data in Flint. This longitudinal population-based measurement of public health in Flint will serve as a marker of current health status, and provide the opportunity to measure population health improvement as evidence-based programs are implemented throughout the city.
Our Phase 1 Scouting results indicate:
-Locating inhabited dwellings for study inclusion in a depopulating city like Flint has major challenges.
- There was utility in having Flint residents trained as data collectors. Harnessing residents’ existing comfort with traversing low occupancy neighborhoods, and allowing them to collect real-time inhabitation data holds significant advantages over other widely used methods. (e.g. relying on aged municipal parcel vacancy data, or using Google Earth observations).
- Houses that FASt data collectors indicated were inhabited could have easily been considered as “uninhabited” via other methods. This could cause residents of ambiguous dwellings (likely to be the most marginalized residents with highest levels of unmet health needs) to be overlooked.
ACKNOWLEDGEMENTS
This project is supported by funding from the National Institute on Minority Health and Health Disparities (3U54MD011227, PI: Furr-Holden). Maps by Christopher Hippensteel, GIS Analyst